SHEIKH FAZILATUNNESSA MUJIB MEMORIAL
KPJ SPECIALIZED HOSPITAL
01810008080.
0244077031.
0244077030.
0244077031.
0244077030.
01810008080.
0244077030. 0244077031.
Search
SHEIKH FAZILATUNNESSA MUJIB MEMORIAL
KPJ SPECIALIZED HOSPITAL
JOURNAL ARTICLE
Vol 1 Issue1 January 2023 Share Share
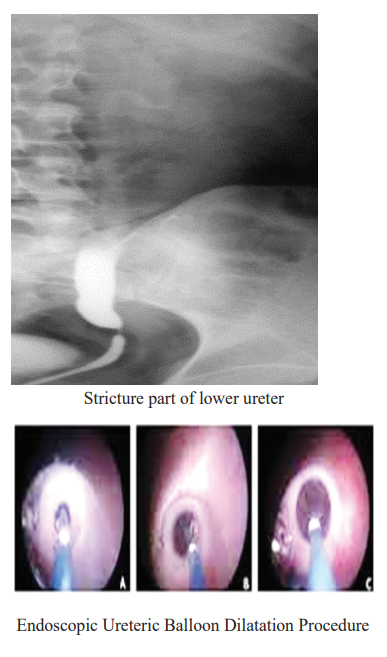
Mr. J, 31 years old, male came in urology OPD with left loin pain radiated to left inguinal area. Patient had history of Tonsillectomy 2012, HTN. O/E: Left lower abdomen was tender, Ext. gent. Normal, DRE-normal. Urine RME & Sr. Creatinine were normal, X-ray LS - Degenerative change of dorsal spine, USG of KUB–Left sided hydronephrosis, IVU-Left sided hydro uretero nephrosis due to stricture of left lower ureter. On 26.11.18 Cystoscopy B/L RGP + Left Lower ureteric dilatation + D-J stenting done under spinal anesthesia, Ureteroscopic evaluation showed fibrotic changes of the ureteral wall. There was no evidence of suspicious lesions or tumors. The ureteroscope did not pass beyond the area of stricture part less than 2 cm). The balloon catheter was placed through narrow ureter along the guide wire, and the balloon was pressurized to 25 atm & Dilated, expansion for 10 min, dilatation performed distally & proximally of stricture part, then D-J stent well kept. The stent was removed 2.5 months later and 3, 6-month & 3 year postoperative US studies showed no hydroureteronephrosis. The patient has remained asymptomatic
No accepted medical treatment of ureteric strictures currently exists. Surgical procedures used in these patients include the following:
Ureteric Stricture – can block or narrow the ureter & making it difficult to pass urine from the kidney to bladder. Ureteric stricture can lead to urinary dilatation, water accumulation, and renal colic in the consensus on balloon type, dilatation pressure, technique. A few large studies, including the 151 cases reviewed by Kuntz and associates.2 Show no long-term sequelae or clinically significant complications from ureteral balloon dilation up to 18F.3 A few studies have demonstrated a 0% success rate at 12 months for endoscopic management of strictures of more than 2 cm at any location. Therefore, more and more urologists choose to treat ureteral stricture under endoscopy. The techniques of urinary endoscopic treatment of ureteric stricture include ureteric balloon dilatation, ureteral holmium laser incision, and ureteral stent implantation. Among them, the ureteric balloon dilatation technique is characterized by the use of a balloon to uniformly force the ureteral wall, tearing the narrow scar tissue, expanding the inner diameter of the ureter, re canalizing the urinary tract, and alleviating hydronephrosis. It have been reported with less complications and simple procedure.
Endoscopic ureteral balloon dilatation for benign ureteric stricture is a better & feasible treatment option in the era of minimally invasive surgery. Its effect can be long-lasting in selected patients, that is, non-irradiated, incidental, short strictures with normal kidneys
1. Endoscopic Management of Ureteral Strictures: an Update. Lucas JW, Ghiraldi E, Ellis J, Friedlander JI.Curr Urol Rep. 2018 Mar 2;19(4):24. doi: 10.1007/s11934-018-0773-4.PMID:29500521 Review
2. Kuntz NJ, Neisius A, Tsivian M, et al. Balloon dilation of the ureter: a contemporary review of out comes and complications. J Urol. 2015;194:413–417. [PubMed] [Google Scholar]
3. Byun SS, Kim JH, Oh SJ, Kim HH. Simple retrograde balloon dilation for treatment of ureteral strictures: etiology-based analysis. Yonsei Med J. 2003;44:273–278. [PubMed] [Google Scholar]